Provider Volunteers
Thank you for your interest in supporting the COVID-19 Public Health Emergency Response.

As a volunteer, you will undergo a pre-screening process prior to being referred to one of the NETCCN clinical teams currently supporting COVID-19 responses. The clinical teams will ask for additional information to confirm your credentials and to assign appropriate roles supporting the COVID-19 response.
During the volunteer on-boarding process, you will be asked to provide at least the following:
- A copy of a current government issued photo ID
- A copy of a second photo ID
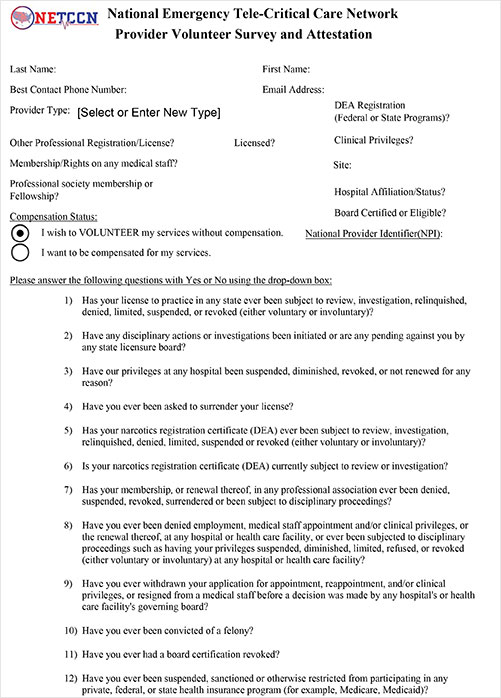
- Your National Provider Identification (NPI) number
- Your active and unrestricted Medical License Number and State of Issuance
- Your valid and active federal DEA registered number
This information will facilitate background checks. Following this process, you will be asked to sign a Volunteer Affirmation Statement to affirm that you acknowledged the minimum expectations of NETCCN volunteers.
Instructions
- Validate that you have a PDF reader with form-completion features.
Need a PDF Reader? Download a PDF Reader by clicking here. - Download the "NETCCN-002-001-A-Provider-Volunteer-Survey-v-0pt3.pdf" form in pdf format.
- Complete the PDF form and save completed survey.
- Email the completed survey to:
usarmy.detrick.medcom-usamrmc.mesg.netccn-operations-officer@mail.mil.